

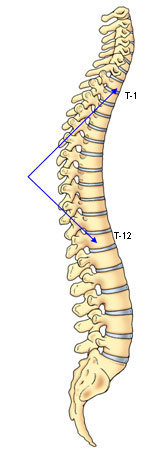
The normal spine, when viewed from behind, appears straight throughout its entire length. However, when one looks at the spine from the side, there are two visible curvatures. There is a gentle rounding of the upper back from the shoulders to the bottom of the ribcage known as thoracic kyphosis and an opposite curve in the lower back known as lumbar lordosis. These two opposite curvatures of the spine are necessary in the normal spine to balance the trunk and head over the pelvis.
A normal thoracic spine extends from the 1st to the 12th vertebra and should have a slight kyphosis ranging from 20o to 45o. When the "roundness" of the upper spine increases past 45o it is called "hyperkyphosis". Scheuermann's kyphosis is the most classic form of hyperkyphosis and is the result of wedged vertebrae that develop during adolescence. The cause is not currently known and the condition appears to be multi-factorial and is seen more frequently in males than females.
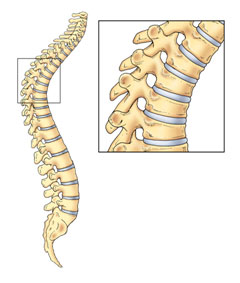
The increased thoracic kyphosis which occurs in Scheuermann's is a rigid deformity. Unlike postural kyphosis, it does not correct when the patient is asked to stand tall or when the patient is asked to bend forward. It is a structural kyphosis that occurs when the front sections of the vertebrae grow slower than the back sections. This results in wedge-shaped vertebrae rather than rectangular shaped vertebrae that line up well (Figure 1). This occurs during a period of rapid bone growth, usually between the ages of 12 and 15. The abnormal kyphosis is best viewed from the side in the forward-bending position where a sharp, angular abnormal kyphosis is clearly visible.
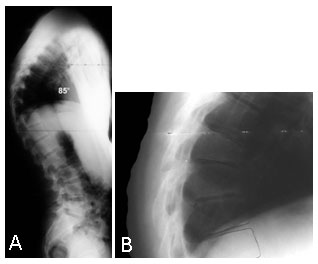
Patients with Scheuermann's disease often present with poor posture and complaints of back pain. Back pain is most common during the early teenage years and in most instances will decrease as they approach adulthood. The pain rarely interferes with daily activity or professional careers. Patients with postural kyphosis have no abnormalities in the spinal vertebrae. However, patients with Scheuermann's kyphosis demonstrate asymmetrical growth of several vertebrae which causes a sharp, rigid angular kyphosis. (Figure 2)
The kyphotic deformity that develops with growth frequently remains mild and requires only periodic x-rays. When the deformity is moderately severe (55o-80o) and the patient remains skeletally immature, brace treatment in conjunction with an exercise program is the recommended treatment.
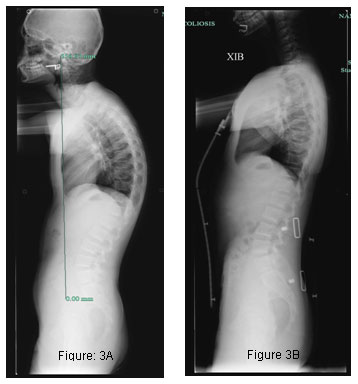
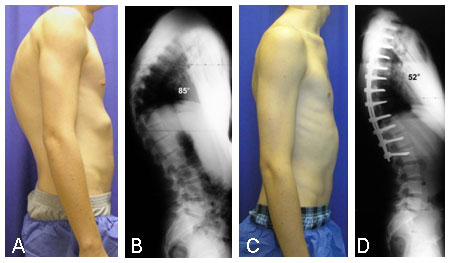
Full time use of a brace (20 hours/day) is usually required initially until maximum correction has been achieved. The brace fit must be regularly evaluated and adjusted to ensure optimal correction. During the last year of treatment prior to skeletal maturity, part time brace wear (12-14 hours/day) may be proposed. Brace wear must be continued for a minimum of 18 months in order to maintain a significant, permanent correction of the deformity. (Figure 3)
When the kyphotic deformity has become severe (greater than 80o) and the patient is often experiencing increased back pain, surgical treatment may be recommended. Surgical intervention allows significant correction to be achieved typically without the need for postoperative bracing. Patients are usually able to return to normal daily activities within 4-6 months following surgery. The correction achieved from surgical intervention is remarkable. (Figure 4)
In most cases, Scheuermann's kyphosis is non progressive and only requires observation and exercise. Others may require bracing until skeletal maturity. However, the more severe (greater than 80o) curves may require surgery.