Congenital Kyphosis
Kyphosis is the forward curvature of the spine—30° to 60° degree curvatures—as seen from the side. If the spine does not form or segments don't separate properly in utero, it can become a sharp angulation that is visible by looking at the skin—called congenital kyphosis.
The spinal cord can sometime become tented over the hump, which can lead to neurologic problems such as:
- Difficulty walking
- Pain in legs
- Difficulty controlling urination
Failure of formation or segmentation are the two basic types of congenital kyphosis:
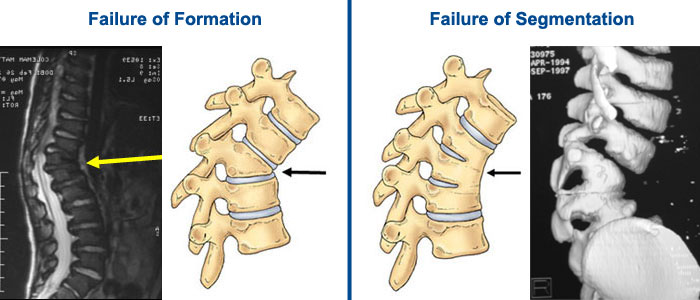
Figure 1. The left images show an MRI of multiple wedged vertebrae depicted in the illustration. The right images demonstrate failure of segmentation. The CT 3D reconstruction shows an example of combined vertebrae.
Treatment Options
Nonoperative Treatments
- Observation with serial examination and x-rays to monitor curvature
- Casting/Bracing is not usually effective for congenital kyphosis. It may delay progression, but evidence for this is not yet available.
Operative Treatments
The surgical choice for progressive congenital kyphosis is a solid fusion of the deformed vertebrae.
- In Situ Fusion: In situ fusion means that the curve will be fused "where it is" with little or no correction of the spine. It is considered a safer fusion surgery.
- Instrumented Fusion Osteotomy: With progressive kyphotic curves in older children, surgery may include instrumentation (rods, hooks, and screws) to help correct the curvature. If the spinal cord is unable to tolerate the manipulative techniques that "straighten" the spine, the surgeon may consider the removal of the misshapen vertebrae to realign the spine.
- Other Osteotomies: Your surgeon may recommend an osteotomy (bone-cutting procedure) to realign the spine.
- Pedicle subtraction osteotomies work by removing the bone in the back of the vertebra so the bone can be collapsed backward.
- Vertebral column resections allow resection of the front and the back of the spine from a posterior procedure.
The surgeon may also recommend separate approaches from the front and the back of the spine.
Prognosis
With the rapid growth of the skeleton in the first year of life, progression is highly likely and there is the potential for spinal cord compression. Failure of separation (segmentation) has a slower rate of worsening and may not become a surgical curve until adolescence.

